Recognising the real diagnosis
Understanding acquired hypothalamic obesity (aHO)
Has a patient you're treating following craniopharyngioma, pituitary adenoma, other (supra)sellar tumours, tumour-related treatments, traumatic brain injury, stroke or hypothalamic inflammation...
...shown clinical features of pathological, insatiable hunger, decreased physical activity and apathy, and/or accelerated and sustained weight gain?
It’s not just obesity.
It could be
acquired hypothalamic obesity (aHO)
The symptoms are clear.
The diagnosis might not be.
When should you consider aHO? Reach out to discuss your specific challenges in recognising and managing aHO

What is aHO and how is it
caused?
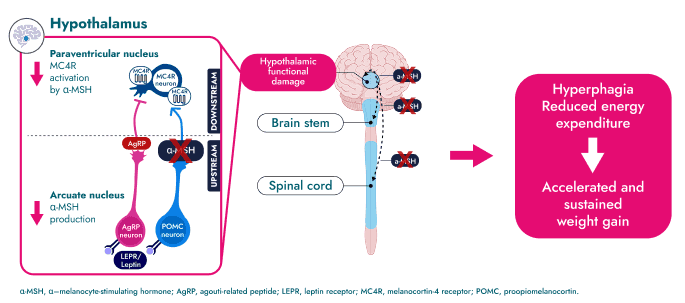
aHO is an accelerated and sustained weight gain resulting from physical injury or structural abnormality of the hypothalamus with melanocortin-4 receptor (MC4R) pathway disruption and other hypothalamic functional impairment.1,2
The MC4R pathway in the hypothalamus is central to energy homeostasis, integrating signals for satiety, hunger and energy expenditure3-5. Structural abnormalities or injury to the hypothalamus can disrupt the MC4R pathway’s control of satiety and energy intake and expenditure, driving accelerated and sustained weight gain in aHO.1,6
The MC4R pathway can become disrupted by a number of aetiologies, such as tumours and their associated treatments, traumatic brain injury, infections, inflammation, stroke and anatomical defects;7-11 however, it is important to note that regardless of the underlying aetiology, patients with aHO typically present with similar clinical features such as hyperphagia, reduced energy expenditure and accelerated and sustained weight gain driven by the MC4R pathway disruption.12
Select your specialty to view associated aetiologies

Expert insight meets real-life experience. Watch this clip of Prof. Dimitri's interview with the parents of a patient living with aHO on their experience.
aHO can cause severe physical
and psychological
complications14,24,25
Which drive significant quality of life impairment for patients and caregivers, as well as leading to early mortality in these suffering and underserved patients with aHO26-28
Physical burden
Significant impact on daily life24,29
Disrupted sleep
Fatigue and decreased physical activity
Lowered physical ability
Accelerated and sustained weight gain
Emotional, social and pathological burden
Affects emotional wellbeing and social connection24,29
Frustration due to difficulty losing weight
Challenges at school
Worse body image perception
Fewer positive social interactions
aHO is a complex disease that has an extensive burden on patients and caregivers. Book a conversation with our team to review practical resources and support that may help you in clinical practice
The MC4R pathway
Learn more about the mechanism of the MC4R pathway, and how impairment can lead to hyperphagia.
Hyperphagia and obesity
in aHO
What is Hyperphagia?
How does it work?
Hyperphagia and obesity in aHO
Hyperphagia and decreased energy expenditure are key clinical features of MC4R pathway disruption, and can drive accelerated and sustained weight gain seen in aHO.14,24,30-34
![]() 72%
72%
Of individuals who had survived craniopharyngioma and were living with obesity, reported hyperphagia (according to a study of tumour-related aHO)24
![]()
Patients with aHO have significantly lower energy expenditure compared with controls with general obesity32-34
![]() 50%
50%
Following hypothalamic injury, approximately 50% of patients with tumours involving the hypothalamic region show BMI increase35
Spot the clinical features often missed.
In this article, Professor Dimitri explores the key clinical features of aHO that are often overlooked
Resources
Do any of your patients show features consistent with aHO?
Let’s connect to discuss possibilities for identification and the practical support available
Stay informed
Sign up to stay up to date on the release of new resources
References:
- 1.
Dimitri P. Front Endocrinol (Lausanne). 2022:10.3389/fendo.2022.846880
- 2.
Gan HW, et al. Endocrine Reviews. 2024;45:309–342
- 3.
da Fonseca ACP, et al. JDC. 2017;31:1549–1561
- 4.
Baldini G and Phelan KD. J Endocrinol. 2019;241:R1–R33
- 5.
Rossi J, et al. Cell Metab. 2011;13:195–204
- 6.
Van Santen HM. Horm Res Paediatr. 2025:10.1159/000543544
- 7.
Hochberg I, et al. Obes Rev. 2010;11:709–721
- 8.
Roth CL, et al. Diabetes Obes Metab. 2024;26:34–45
- 9.
Cerbone M, et al. E Clinical Medicine. 2020:10.1016/j.eclinm.2019.11.017
- 10.
Nannette G, et al. J Clin Endocrinol Metab. 2023;108(2):323–330
- 11.
Roth CL, et al. Obesity (Silver Spring). 2015; 23:1226–1233
- 12.
van Santen HM, et al. Diabetes, Obesity and Metab. 2026; doi:10.1111/dom.70725
- 13.
Garnett MR, et al. Orphanet J Rare Dis. 2007;2:10.1186/1750-1172-2-18
- 14.
Van Santen HM and Muller HL. Endocr Rev. 2025:10.1210/endrev/bnaf025
- 15.
Ruiz S et al. Eur J Endocrinol. 2022;186(6):R79–R92
- 16.
Madsen PJ, et al. J Neurosurg Pediatr. 2019;24(3):236–245
- 17.
Maas AI, et al. Lancet Neurol. 2008;7(8):728–741
- 18.
Crenn P, et al. Clin Nutr. 2014;33(2):348–353
- 19.
Mele C, et al. Int J Mol Sci. 2021;22:10.3390/ijms22052686
- 20.
Jais A and Bruning JC. J Clin Invest. 2017;127:24–32
- 21.
Goszyonyi G, et al. Brain Structure and Function. 2020;225:1459–1482
- 22.
Etemadifar M, et al. Care Rep Med. 2012:10.1155/2012/768580
- 23.
Hietamäki J, et al. E Clinical Medicine. 2022;51:101556
- 24.
Kayadjanian N, et al. J Clin Endocrinol Metab. 2023;109:e75–e87
- 25.
Chandrasekaran P and Weiskirchen R. J Cell Commun Signal. 2024;18(2):e12039
- 26.
Müller HL, et al. Sci Rep. 2025;15:2118
- 27.
Van Santen HM, et al. Eur J Endocrinol. 2023;188:10.1093/ejendo/lvad009
- 28.
Shoemaker AH, et al. Impact of Setmelanotide on Metabolic Syndrome Risk Score in Pediatric Patients With Acquired Hypothalamic Obesity. Presented at: Pediatric Endocrine Society; 2025; National Harbor, MD, USA
- 29.
Craven M, et al. Front Endocrinol (Lausanne). 2022;13:876770
- 30.
Argente J, et al. Rev Endocr Metab Disord. 2025;10.1007/s11154-025-09984–3
- 31.
Harz KJ, et al. J Clin Endocrinol Metab. 2003;88:5227–5231
- 32.
Abawi O, et al. Front Endocrinol (Lausanne). 2022;13:862817
- 33.
Bomer I, et al. J Pediatr Endocrinol Metab. 2015;28(11–12):1305–1312
- 34.
van Schaik J, et al. Endocr Connect. 2022;11(8):e220276
- 35.
Hulsmann SC, et al. Endo Connect. 2025;14:e240533